
Because surgery and radiation can cause significant changes in one’s quality of life, it’s important to gain some basic knowledge of the anatomy. It’s also important to ask your doctor about how your treatment plan might impact basic functions such as eating, swallowing, smell, taste and more. Before and during treatment, ask your physician about resources that might be available during recovery. Resources might involve the services of a dental oncologist, nutritionist, speech therapist, pain management specialist, pharmacist and more.
Approximately 80% of ACC patients are diagnosed with a primary tumor in the head or neck region. ACC of the salivary glands, the most common form of the disease, is thought to account for 25% of all salivary gland malignancies. For this reason, this section will focus on these specific areas of the anatomy.
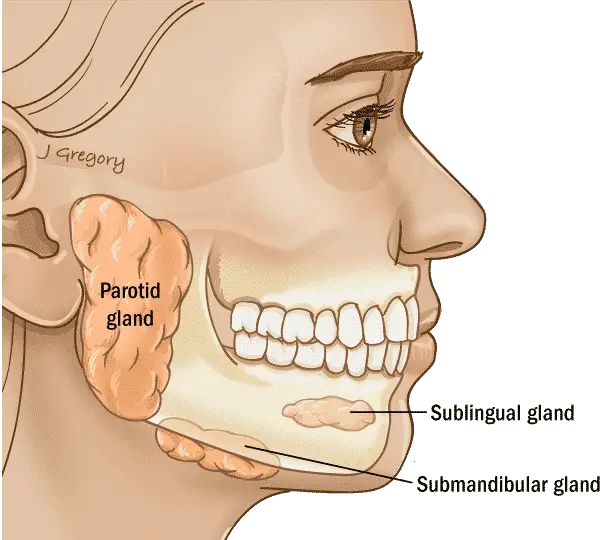
In the head and neck, there are two main types of salivary glands: major salivary glands and minor salivary glands. ACC is often diagnosed in one of the three major salivary glands (parotid, submandibular, sublingual gland) but more than half of ACC cases arise from the minor salivary glands which surround the hard/soft palate, inside the cheeks, nose, sinus, tongue, larynx, pharynx and more.
The 3 Major Salivary Glands
The three major salivary glands are the parotid glands, the submandibular glands and the sublingual glands. These glands produce most of the saliva in your mouth. Saliva helps with breaking down food, swallowing and chewing. It also helps prevent tooth decay and infections from developing in your mouth or throat. The glands in the face and neck are symmetrical, meaning that there is one of each on either side of the face and mouth.
Parotid Salivary Glands
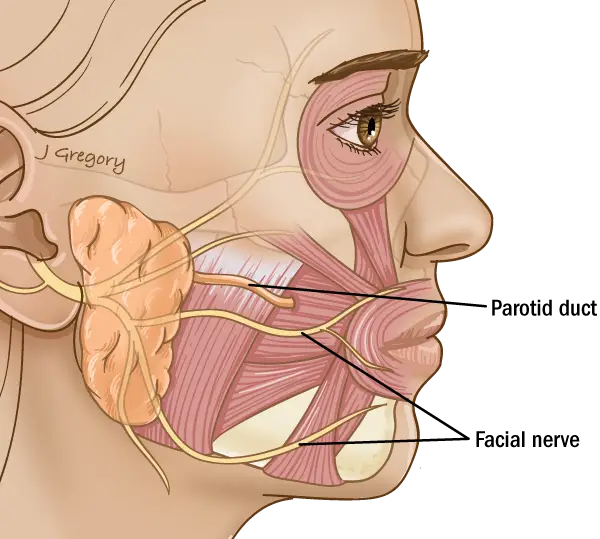
The parotid glands are the largest salivary glands and sit just in front of each ear. Most salivary gland tumors start here.
Each parotid gland has two parts: the superficial lobe and the deep lobe. Between the two lobes is the facial nerve that controls movement of the face. The facial nerve forms multiple branches controlling muscles that give you the ability to close your eyes, raise your eyebrows, smile and more. Other critical structures near the parotid glands include the external carotid artery, which is a major supplier of blood to the head and neck region, and the retromandibular vein, a branch of the jugular vein.
Surgery to treat a parotid gland tumor is called a parotidectomy. Preserving the facial nerve is an important priority when removing a parotid gland tumor. There is a chance that the nerve may be adversely affected by the tumor or by the surgical procedure needed to remove the tumor. The type of parotidectomy is based on the tumor size or the nerves involved.
The Submandibular Glands
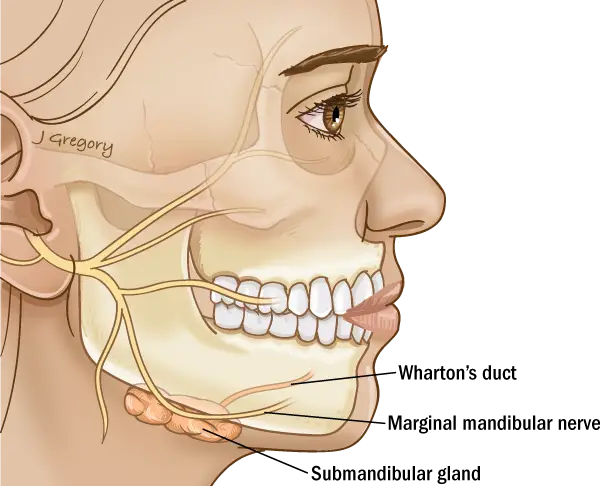
The submandibular glands are located below the jaw and are about the size of a walnut. The saliva produced in these glands is secreted into the mouth from under the tongue.
One of the branches of the facial nerve runs just over the top of the submandibular gland and is called the marginal mandibular nerve. This nerve controls the lower lip and helps you smile. Other nearby nerves may involve areas such as the tongue that help with speech, swallowing (the hypoglossal nerve) and sensation (lingual nerve).
Surgery for tumors in the submandibular gland may involve removal of the entire gland.
A surgeon will make a cut (an incision) under the jawline to remove the gland and some of the surrounding tissue. Again, a submandibular gland excision requires precision on the part of your surgical team due to important nerves nearby.
Sublingual Salivary Glands
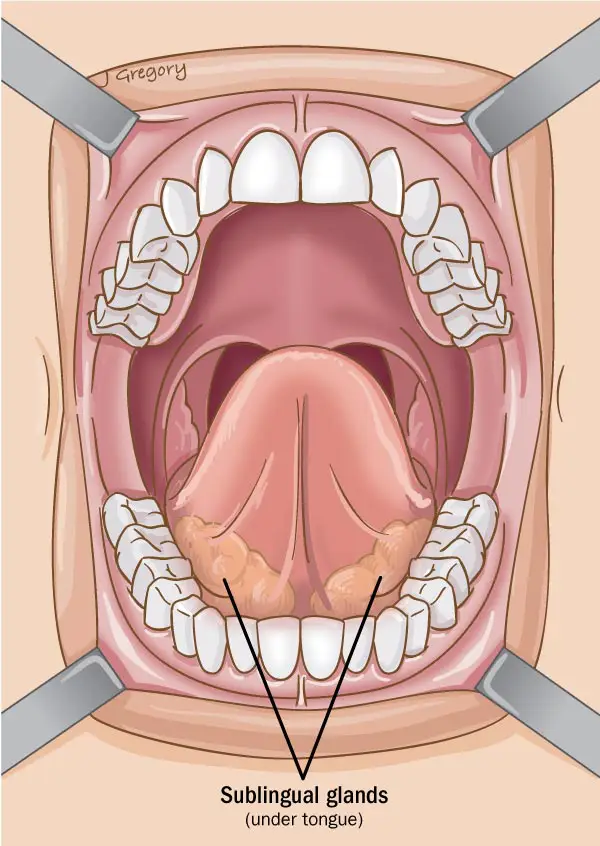
The sublingual glands are the smallest of the major salivary glands and sit on the floor of the mouth and under either side of the tongue. The lingual nerves, which provide sensation to the sides of the tongue, run in very close proximity to these glands. The saliva-carrying ducts from these glands open directly into the mouth.
Surgery for tumors in a sublingual gland may involve removal of the entire gland. A surgeon may make a cut (an incision) inside your mouth to remove the gland along with some of the surrounding tissue. The surgical area is often repaired by either closing the gap with stitches (sutures) or grafting the skin.
Again, the surgery requires precision on the part of your surgical team because the lingual nerve is nearby. The lingual nerve controls feeling and taste on the side of the tongue. The surgical team will preserve the lingual nerve whenever possible.
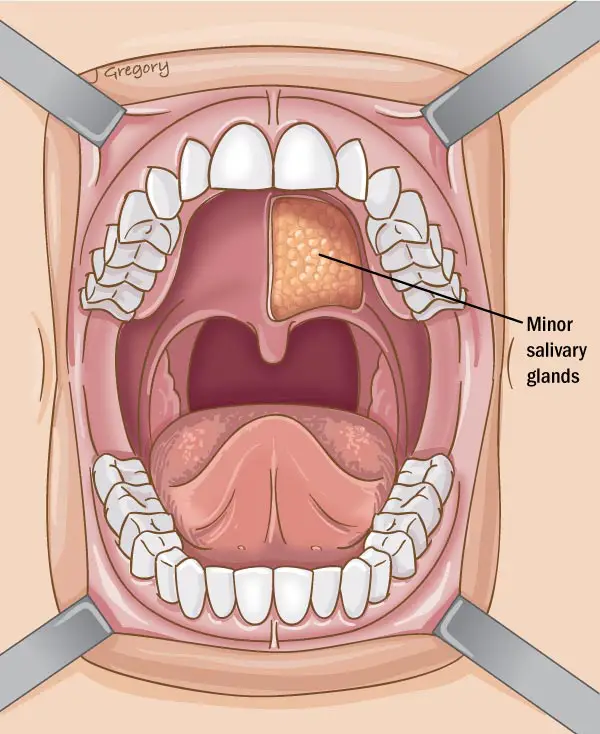
The Minor Salivary Glands
More than half of patients with ACC are diagnosed in the minor salivary glands; with the hard palate being the most commonly affected area of the mouth. These glands are much smaller than the major salivary glands. These glands are located throughout the mouth, the tongue, hard and soft palate, inner cheek, throat, voice box (larynx), trachea, nose, and sinuses.
The primary goal of surgery is to remove all of the visible tumor along with a clear margin of healthy tissue surrounding the tumor. Patients should discuss the surgical plan with their physicians to determine short and long term side-effects, quality of life changes and additional options if available.
Types of minor salivary gland surgeries:
- Glossectomy (Tongue)
- Laryngectomy (Voice Box)
- Maxillectomy (Maxillectomy Types)
- Palate Resection (Hard & Soft Palate)
- Pharyngectomy (Pharynx)
- Craniofacial Resection (for access to tumors between the face and skull base -sinuses/orbit)
- Orbital Cavity & Lacrimal Tearing Structures Only
